
Here is a copy of the presentation from the session given to year 5 Medicine students, February 2017 : year-5-presentation-ferguson-2017-b. Please send me your comments or further questions or put down a comment on this web posting!
Here are the pre-session quiz questions and commentary [thanks all for your answers and well done with the knowledge you displayed! ] :
- What class of antibiotic is vancomycin?
Answer – it’s a glycopeptide
There are a limited number of classes and it is useful to know them as various things are shared within a class- dose routine, toxicity, type of action and resistance . For more, see this posting on our antibiotic stewardship site.
- Main mechanism by which Staphylococcus aureus becomes resistant to penicillin (a betalactam)?
Answer – betalactamase
There are 4 main mechanisms by which bacteria avoid the action of antibiotics. Destruction of the drug (e.g. betalactamase) also occurs as a mechanism for chloramphenicol and aminoglycoside resistance. For many antibiotics, including betalactams , more than one mechanism may be relevant. See this posting for more about S. aureus resistance. Staph. aureus is a really important bug to know something about!
- What is/are the primary aim(s) of antimicrobial stewardship (AMS)?
Answer – all three of the above .
Have a read of this posting to learn more about the three elements of AMS and the Tragedy of the Commons.
- According to PNG Adult medical Standard Treatment Guide, what is the initial dose recommended for gentamicin (an aminoglycoside)?
Answer – 5-7 mg/kg IV
Gentamicin is one of the most important antibiotics for treating aerobic Gram negative infections – e.g. due to E. coli, Klebsiella and other related species. Knowing how to use aminoglycosides safely is very important – there is a narrow therapeutic index – renal and ototoxicity (balance impairment) may result.
Conversely as bacterial killing is concentration dependent, giving a sufficiently high dose in patients who have severe sepsis is important . Toxicity mostly relates to prolonged usage and in Australia, gentamicin is stopped after 48 hrs = maximum of 3 daily doses. If further Gram negative cover required then another class is selected, based on the susceptibility of the infecting isolate.
See this posting on safe use of aminoglycosides. GO here to access online versions of current PNG STGs.
- What is the drug of choice for a methicillin-susceptible Staphylococcus aureus (MSSA) causing a bloodstream infection (BSI)?
Answer- Flucloxacillin IV
A BSI from S. aureus is a serious problem – patients present from the community or it can be a healthcare-associated event and the mortality at one month can be as high as 30%. The most important susceptibility to check is whether the isolate is methicillin-susceptible. If it is, then the best antibiotic to use is flucloxacillin (a betalactam that is not destroyed by betalactamase). It is given by the intravenous route at high dose as a proportion of patients already have endocarditis. For an overview of 10 essential clinical care steps for managing patients with Staph. aureus BSI, see this posting.
- The recommended first line treatment for non-severe Clostridium difficile diarrhoea is:
Answer- Metronidazole oral or IV
There is not much knowledge if any about the incidence of Clostridium difficile infection in PNG to date. Research definitely needed. It is not mentioned in the STGs! A summary of Australian treatment guidance is here.
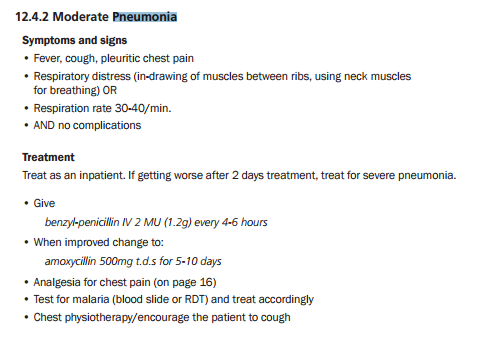
- According to the PNG adult STG, what is the recommended IV treatment for moderate severity community-acquired pneumonia?
Answer- benzyl-penicillin (crystapen) : here is an excerpt –
- What weight is used for calculation of gentamicin dosing ?
Answer – ideal body weight
See this posting for more discussion.
- What puzzles you about antibiotics and their use? [we hope to answer these in further postings at idmic.net – please enrol your email to the website and stay tuned!
- antimicrobial resistance and mechanisms
- not knowing which drug to give exactly for a clinical problem
- new micro-organisms with resistance
- ever changing recommended treatments due to resistance
- which antibiotics are best for which organism
- everything – we’d like more lectures on antibiotics so that we can really master it
- patient being given 3-4 antibiotics at once – why is that done for certain illnesses?
- Do antibiotics only affect bacteria or other organisms as well?
- Why do we substitute antibiotics when the recommended ones are available?
- Dosage of various antibiotics
- Why resistance
- Adjustment in dosage to reach efficacy level
