Pre-analytical issues
- Correct indication for testing – concept of ‘diagnostic stewardship’
- Patient identification and sample labelling
- Correct specimen collection- avoid contamination- esp. blood culture
- Correct transport and storage
- Reject poor samples – sputum with no PMNs squames++, urinary catheters, wound drains, other
Analytical
- Media and reagent Quality Control (QC)
- Antimicrobial Susceptibility Testing QC
- External Quality Assurance (EQA)
- Standard Operating Procedures, staff training and competency assessment
Post-analytical
- Timely reporting with efficient communication and storage of results
- Direct clinical liaison for critical results- positive blood cultures, CSF etc
- Comments to help interpret results – colonisation/contamination vs significant isolates, AST results – extrapolations , cascade reporting, therapeutic advice derived from standard treatment guidelines
References
- WHO Quality Laboratory Manual 2011
- Quality management (IDMIC links)
- ISBAR and clinical liaison process
Identification process
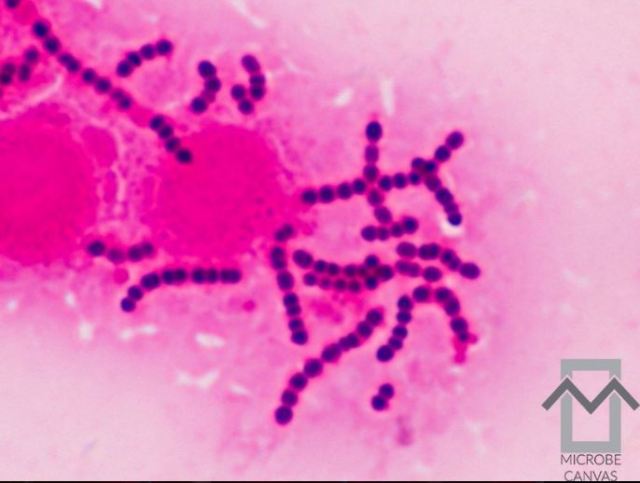
- Presumptive ID characters – Gram stain appearance, culture growth characteristics and colony appearance etc
- Confirmatory ID – biochemical, AST, serological or molecular methods usually; often cannot rely on a single biochemical parameter – e.g. optochin susceptibility for pneumococcus or mannitol fermentation for Staph. aureus– approx. 5% of strains will be atypical and not show the expected result!
Phenotypic methods
- Point of Care (POC) methods – ICTs etc, microscopy is also a potential POC (rapid) test – e.g. gonococcus smear in STD clinic or a pus smear from an abscess
- Microscopy
- Culture
- Rapid tests – indole, catalase, oxidase etc
- Biochemistry kits- API, VITEK
- Antimicrobial susceptibility- some intrinsic resistance characters help to identify bacteria- e.g. all Gram negatives are vancomycin resistant
- Latex Particle Agglutination – e.g. Lancefield grouping for betahaemolytic streptococci
- MALDI-TOF (mass spectrophotometry)
Genotypic methods
- POC methods – PCR based- different formats – LAMP, GenXpert etc
- Conventional PCR – e.g. presence of nuc gene in species indicates it is Staph. aureus
- Sequencing – ribosomal 16S variable regions sequenced to locate signature sequences associated with specific bacterial species (18S sequencing for fungi)
- MLST typing– global and local epidemiology – eg. ESBL ST131 coli , KPC carbapenemase-containing ST258 Klebsiella pneumoniae
- Whole genome sequencing of isolate(s)– can be used to provide an in silico MLST or survey of resistance genes