
What is included as part of Standard Precautions?
SP protect healthcare staff and patients from infection transmission via Direct or Indirect contact modes. The assumption is made that all blood/body fluids are potentially infectious and PPE measures should be taken by staff during healthcare to avoid exposure to bare skin or mucous membranes.
Respiratory hygiene, cough etiquette and the addition of physical (social) distancing measures mean that Standard precautions also reduce transmission via respiratory droplets from an infected person.
COVID-19 note: well-observed SP provide provide protection from contact and droplet transmission whatever the status of the patient and across all modes of healthcare delivery. They are the starting point – if SP cannot be followed properly, then use of vertical (selective) additional transmission-based precautions (gowns, gloves, eye protection and mask) will only have a partial protective effect for staff.
Hand hygiene (World Health Organisation 5 Moments for Hand hygiene Standard) remains a critical priority in the WHO Clean Care is Safer Care program.
Asepsis – conducting invasive and other key procedures with proper regard to Asepsis is critical and applies to all care settings including non-surgical procedures such as preparation of IV medication or insertion of an IV cannula.
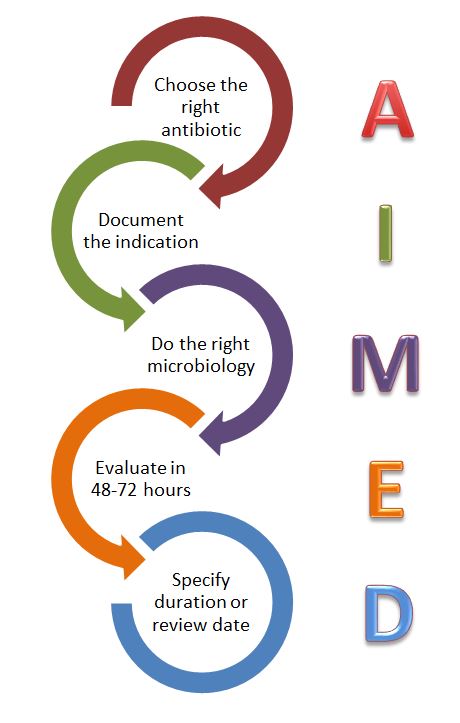
Australia specifies 8 key elements for SP – see poster below. Other ‘Standard Precautions’ that apply across all settings and patients include:
- safe handling and transport of laboratory specimens
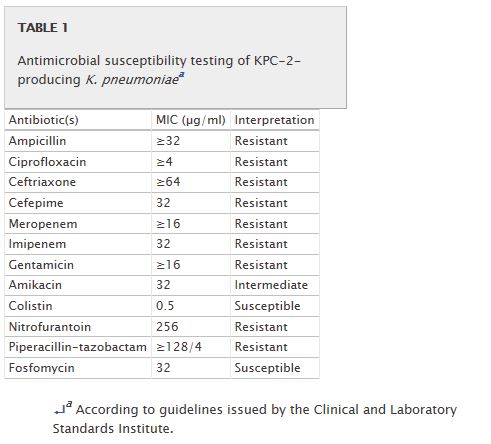
- antimicrobial stewardship
- immunisation
- healthcare-associated infection surveillance and analysis of risk across the healthcare system
- safe hospital design, including ventilation
References
- Critical WHO Guidance (19/3/20): Infection prevention and control during health care when COVID-19 is suspected
- Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings, 2007 Web reference point
- Australian National Infection Control Guidelines- includes links to standard precaution posters





Infectious diseases 101
Some thoughts to stimulate discussion!