Guest posting: Dr Melanie-Anne John, Microbiology Registrar, Pathology North, formerly Infectious Disease Department, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, RSA
Cryptococcal meningitis (CCM) has a high mortality (20-50%) in patients with AIDS. CCM is preventable with fluconazole and is a recommended intervention in patients with a CD4 < 100 cells/ul. Early HAART programmes record high mortality (8-26%) and 20% of these deaths are due to CCM where IRIS may be implicated. Patients entering health services with severe immunocompromise may be tested before HAART is commenced.
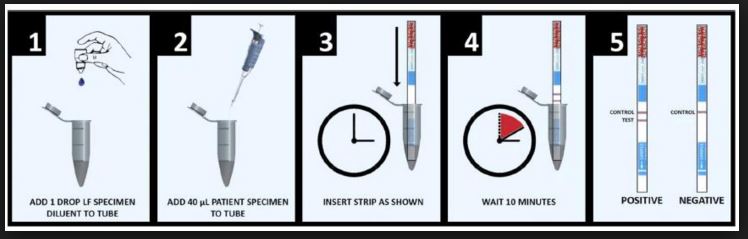
Cryptococcal antigen (CRAG) is detected by latex agglutination (LA) and enzyme immunoassay (EIA) in the laboratory. The development of a rapid test using a lateral flow assay (LFA) has brought this test into the clinic at an affordable cost. The LF has a high sensitivity (83-98 %, specificity 97%). False positives are infrequent and associated with titer
In Africa 13% of patients with CD4 100 days in 11%) before the onset of symptoms.
WHO recommends the LFA as it is cost effective and far below the GDP of most Sub Saharan countries. Cost effect varies by region but remains under 14 USD/life saved where CRAG + prevalence is >2%.The actual cost is of each test is 3.97 USD compared with 206 USD to treat one case of CCM.
Pre-emptive therapy is an attractive consideration in patients with CD4<100/ul and titre > 8, then only 52 tests are required to identify 1 case.
Patients should be screened before testing : including a history of CCM as antigen can be detected for long periods after successful treatment in the immunocompromised as well as for current symptoms of meningitis.
A positive LFA should trigger a lumbar puncture but in poorly resourced clinics, fluconazole may be commenced and the patient is then referred for lumbar puncture.
Caveats
- Test and treat LFA is not recommended for children and adolescence due to low prevalence of disease.
- For a true bedside test, whole blood finger prick specimen is best. LFA is under evaluation for this.
- Consider as a laboratory reflex test for cryptococcal antigen when a CD4 count is detected
Reference
- CDC (USA) Resource page , cryptococcal meningitis prevention
Picture: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0036-46652015000800038

Pingback: Cryptocococcal infection bibliography – PNG and Cambodia | Microbiology and Infectious Diseases postgraduate teaching