It’s important to understand as much as you can about Staphylococcus aureus – it is such a prevalent cause of community and healthcare-associated infection and remains a major challenge to control. It’s not just one species – various clones of MSSA and MRSA dominate across parts of the world and within subpopulations for reasons that are not always apparent despite much deep research into organism sequences and putative virulence gene expression. Always important to keep in mind that the epidemiology of S. aureus will vary in different locations according to what specific strains are prevalent. Critical host factors that make disease more likely are also still in dispute – watch this space!
The main way that Staphylococcus aureus (MRSA) strains are described is by use of MLST (multi-locus sequence typing) and SSCMEC typing (this link is to the International Working Group on the Staphylococcal Cassette Chromosome elements). There are three elements in the description- e.g. ‘ST239-III-MRSA’- the sequence type (239) is followed by the SSCMEC type (III) and then whether the isolate is MRSA (mecA positive) or MSSA (mecA negative). The field guide reference below gives you the detail.
Annotated schema from Nature Reviews 2009 paper:
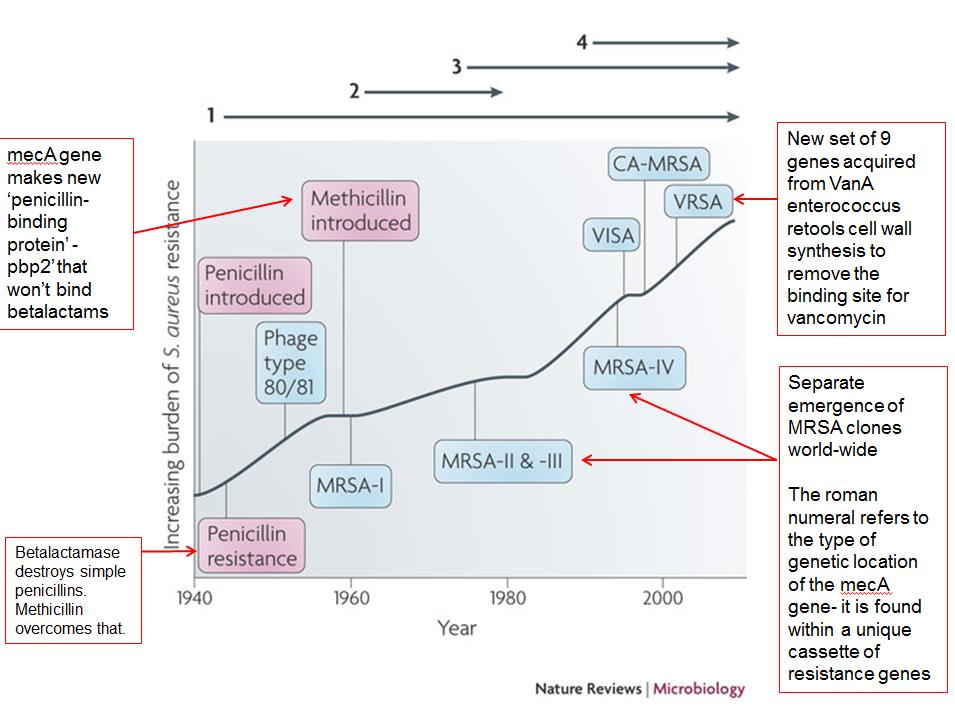 Wave 1 (indicated above the graph), which continues today, began shortly after the introduction of penicillin into clinical practice in the 1940s. The first pandemic antibiotic-resistant strains, from the lineage known as phage type 80/81, were penicillin-resistant and produced Panton–Valentine leukocidin (PVL).
Wave 1 (indicated above the graph), which continues today, began shortly after the introduction of penicillin into clinical practice in the 1940s. The first pandemic antibiotic-resistant strains, from the lineage known as phage type 80/81, were penicillin-resistant and produced Panton–Valentine leukocidin (PVL).
Wave 2 began almost immediately following the introduction of methicillin (a betalactamase-stable penicillin) into clinical practice with the isolation of the first MRSA strain (an archaic clone), which contained staphylococcal chromosome cassette mec I (SCCmecI) (indicated on the graph as MRSA-I); this wave extended into the 1970s in the form of the ‘Iberian clone’.
Wave 3 began in the mid to late 1970s with the emergence of new MRSA strains that contained the new SCCmec allotypes, SCCmecII and SCCmecIII (MRSA-II and MRSA-III), marking the ongoing worldwide pandemic of MRSA in hospitals and health care facilities. The increase in vancomycin use for the treatment of MRSA infections eventually led to the emergence of vancomycin-intermediate S. aureus (VISA) strains.
Wave 4, which began in the mid to late 1990s, marks the emergence of MRSA strains in the community. Community-associated MRSA (CA-MRSA) strains were susceptible to most antibiotics other than -lactams, were unrelated to hospital strains and contained a new, smaller, more mobile SCCmec allotype, SCCmecIV (MRSA-IV) and various virulence factors, including PVL. Vancomycin-resistant S. aureus (VRSA) strains, ten or so of which have been isolated exclusively in health care settings, were first identified in 2002.
SSCmec cassettes are derived from coagulase negative staphylococcal species. The initial clones of MRSA (with types I, II or III SSCMEC) were generated by a very small number of transfer events leading to just a handful of ‘archaic clones’. With later, smaller, more transferable cassettes such as IV, there have a been a much more diverse range of new MRSA strains emerging.
References
- Waves of resistance: Staphylococcus aureus in the antibiotic era, Chambers et al, Nature Reviews 2009
- A Field Guide to Pandemic, Epidemic and Sporadic Clones of Methicillin-Resistant Staphylococcus aureus. 2011 Monecke et al.
- Multilocus sequence typing and the evolution of methicillin-resistant
Staphylococcus aureus. Robinson 2004 et al.
