
Please remember to revise this page for the detailed explanations about AST, MICs, Breakpoints, ECOFFs etc. A summary of relevant concepts is here – Antimicrobial susceptibility testing practical approaches to quality control Nov 2016.
Some questions that arose in today’s tutorial-
1. Is the ECOFF the same as the Clinical Breakpoint MIC?
Not infrequently – for instance, clinical breakpoints are not established for tuberculosis drugs and the ECOFF is used as the breakpoint. And so the isolates with MICs above the ECOFF are assumed to be resistant. However that may not actually be the case- higher dosing may enable higher drug levels and clinical effectiveness.
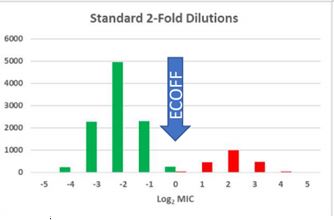
Here we have a nice separation of wildtype (green) and non -WT (red) isolates with an ECOFF (at the upper limit of the WT distribution) that separates the two well. When clinical breakpoint setting takes place, the first issue that is taken into account is the ECOFF – the clinical breakpoint must not be set to a value that lies within the WT distribution. If it is, then the same WT isolate may test resistant or susceptible on successive tests due to the inherent variability of testing.
2. Can an ECOFF be always discerned from the MIC distribution?
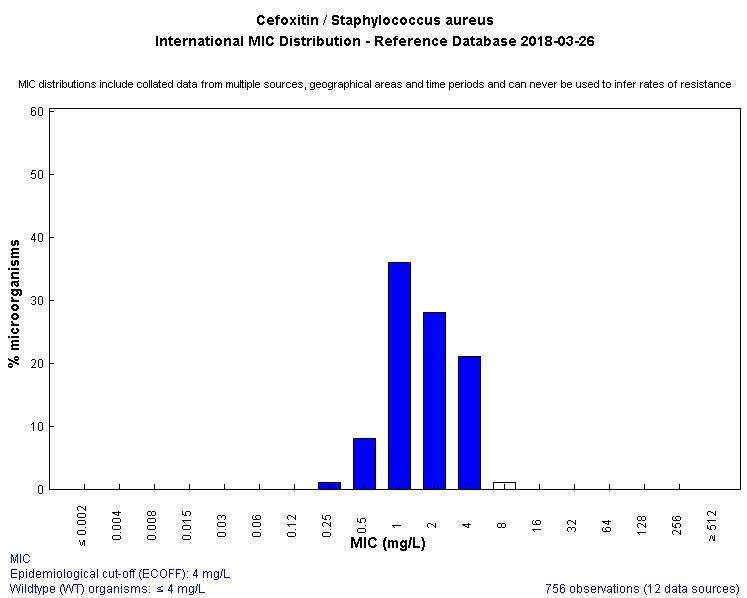
No- take a look at this distribution- the nonWT (red) isolates have a different MIC distribution but this overlaps the WT distribution. There is no MIC value that will separate the two populations. In this circumstance , provided the clinical breakpoint can be set above both distributions (i.e. achievable drug levels and PD parameters can be satisfied for isolates 2 or below) then there is no problem. Or perhaps a different antibiotic will allow the separation of WT and Non-WT – a good example is MRSA detection – the MIC distributions of MRSA and MSSA overlap when tested against oxacillin. When tested against cefoxitin, they dont overlap. See the following two graphics – WT is blue.


3. What quality control is necessary for AST? What are possible reasons for smaller or larger zones than expected when testing control organisms? How should one handle the control (ATCC) strains to ensure that they work properly?
Fiona’s presentations take you through what you need to know – please review them via here.
4. We discussed the three antimicrobial agents for this module – flucloxacillin, amoxycillin/clavulanate and cotrimoxazole (bactrim) which you need to systematically study. I asked whether Strep. pyogenes is ‘susceptible’ to cotrimoxazole (SXT)?
This recent paper provides one answer – S. pyogenes‘ in vitro susceptibility to SXT depends on the medium’s thymidine content and provided that is controlled, nearly all isolates are susceptible. There was a subsequent letter and reply which challenged the presumption that thymidine content in tissue may be sufficient to render SXT resistant in practice; however that is an issue that cannot be decided yet.
SXT remains useful for MSSA and MRSA treatment – the 2016 PMGH antibiogram showed 96% and 91% susceptibility for MSSA and MRSA respectively. Gram negative susceptibility unfortunately very low now.
This graphic about emergence of resistance in Staph. aureus is useful – Staph aureus resistance.
Please contact me with any other questions re this important topic. I will post a separate posting with questions on interpreting the cumulative antibiogram later this week. John
