
Guest posting: Dr Ian Marr, Microbiology Registrar, Pathology North.
Melioidosis is a cause of severe pneumonia, bacteraemia, urosepsis, prostatic abscess, CNS infection, pyogenic myositis and liver and spleen abscesses. It is found in PNG especially around the Balimo region – see Warner, Currie et al 2018 : Melioidosis in Papua New Guinea and Oceania- an important short read.
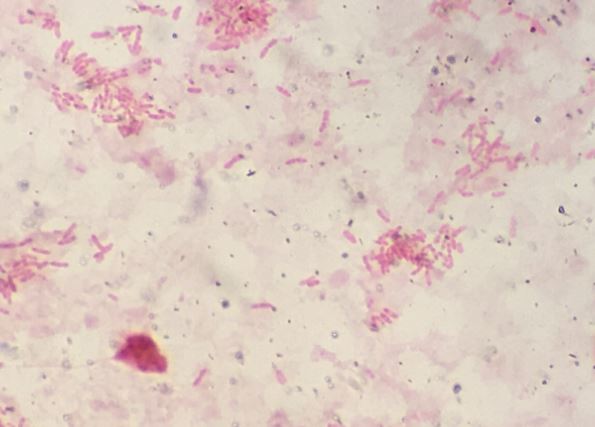
Melioidosis is caused by Burkholderia pseudomallei, a Gram-negative rod, straight or slightly curved, with bipolar staining (below), or safety pin appearance. It is highly motile when viewed under phase contrast microscopy.
It is intrinsically resistant to colistin and gentamicin and therefore can be isolated on selective media containing these agents.
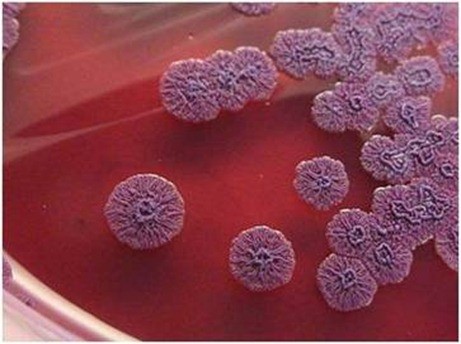
The best media for this is Ashdowns. This enables the other organisms to be suppressed and not overgrow Burkholderia (needed when isolates are from non-sterile sites).
Ashdown’s media contains:
- Trypticase soy agar
- Crystal violet – inhibits Gram positive organisms
- Gentamicin – inhibits many Gram negative organisms (except B. pseudomallei)
- Neutral red – absorbed by B. pseudomallei to differentiate from other bacteria
- 4% glycerol – required by some B. pseudomallei strains for growth
- Look for the characteristic flat wrinkled purple colonies by 48h
Other features include:
- Strict aerobe, non lactose fermenter on MAC agar
- Earthy odour (but important NOT to smell plates as this can cause laboratory acquired infections)
- Catalase +ve, oxidase +ve
- MALDI – there are limitations to using (MS) mass spectrophotometry currently. Often times it is mis-identified unless you have access to the security sensitive database on the Bruker, or you have your own curated library for this organism.
- Can be misidentified by Vitek 2 (called B. cepacia, or thialandensis for instance)
- API-E and NE can also mis-identify this organism
- Australia sites where there is a lot of this organism use PCR targets (type III secretion system)
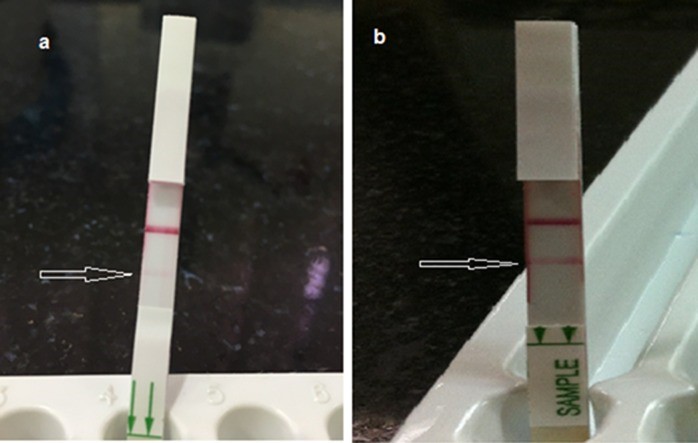
- NEW* – Lateral flow assay – developed by InBios
- 99% sensitive and 100% specific on positive BC samples
- Place a drop of blood in with extraction mixture for 2-3min and then apply this solution to the lateral flow device. See this paper for recent trial in Laos.
Issues with handling:
- RG2 (Risk Group 2) organism; laboratory-acquired infection reported so DO NOT USE AEROSOLISING PROCEDURES
- Work in a biological safety cabinet; use appropriate PPE; avoid sniffing plates
- Bactrim prophylaxis (3 weeks) for high-risk exposures; monitor for symptoms & seroconversion
Treatment / Antibiotic susceptibility
- High mortality – especially when immunosuppressed, diabetic, renal failure.
- Intrinsic resistance to: penicillin, aminoglycosides, macrolides, colistin
- Usually susceptible to: ceftazidime, meropenem, TMP-SMX-> augmentin and doxycycline used as second line agents
- AST by disc diffusion is unreliable
- E-test to determine MIC is necessary: TMP-SMX, meropenem, ceftazidime, doxycycline
- Treatment: generally, 14-28 days IV ceftazidime, then >=3 months of oral eradication (TMP-SMX) depending on site of infection – See Royal Darwin Treatment 2014 guidelines.
