
Here are example antibiograms for Hunter New England (NSW). These are constructed by assessing the % susceptible for specific bugs and drugs, taking only the first isolate of a species per person per annum. Where is it possible extrapolate susceptibility rather than test or we know a particular species is intrinsically susceptible, we enter “S”. Conversely, species that are intrinsically resistant to an antibiotic (e.g. Gram negatives and vancomycin) are marked as “R”. In either situation, there is no rationale for actually testing that antibiotic against the species.
Nocardia and aerobic actinomycetes
Guest posting: Dr Syeda Navqi, Microbiology Registrar, Pathology North.
Group: Aerobic actinomycetes
- Gram positive bacteria that are usually filamentous and branched, commonly producing a fungus like mycelium that fragments into rod shaped or short coccoid form.
- All grow better under aerobic than anaerobic conditions, a feature distinguishing them from most organisms in the genus Actinomyces.
- The organisms containing mycolic acids in their cell walls (included in the genera Nocardia, Rhodococcus, Gordonia, Tsukamurella, and Corynebacterium) are rather closely related on the basis of molecular genetic studies. c.f. Streptomyces, Actinomadura, Dermatophilus have no mycolic acid.
- Nocardia is the most important genus as the most commonly isolated aerobic-actinomycete human pathogens.
- There are approximately 87 validly named species included in Nocardia genus.
Identification
Posted in Bacteria (GPOS), Med Micro topics-advanced, Module-Respiratory infections
Tagged Nocardia
Leave a comment
Recent update on TB diagnostic techniques – GenXpert MTB/RIF Ultra
Guest posting: Dr Ian Marr, Microbiology Registrar, Pathology NSW, Hunter
The GenXpert used in most LMIC has cartridges for detection of Mycobacterium tuberculosis (MTB) – GenXpert MTB/RIF. These contain primers and molecular beacon probes for the detection of both MTB and its resistance to the first line drug rifampicin. By looking for mutations in the rpoB gene (transcribes for RNA polymerase) it can determine if rifampicin (which inhibits RNA polymerase) will work and also if MTB is present. Continue reading
AST, MIC, Clinical Breakpoints, ECOFFs and AST QC
Please remember to revise this page for the detailed explanations about AST, MICs, Breakpoints, ECOFFs etc. A summary of relevant concepts is here – Antimicrobial susceptibility testing practical approaches to quality control Nov 2016.
Some questions that arose in today’s tutorial-
1. Is the ECOFF the same as the Clinical Breakpoint MIC?
Not infrequently – for instance, clinical breakpoints are not established for tuberculosis drugs and the ECOFF is used as the breakpoint. And so the isolates with MICs above the ECOFF are assumed to be resistant. However that may not actually be the case- higher dosing may enable higher drug levels and clinical effectiveness.
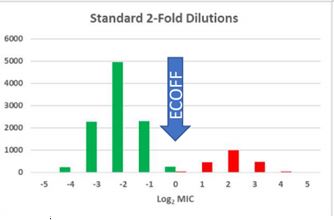
Here we have a nice separation of wildtype (green) and non -WT (red) isolates with an ECOFF (at the upper limit of the WT distribution) that separates the two well. When clinical breakpoint setting takes place, the first issue that is taken into account is the ECOFF – the clinical breakpoint must not be set to a value that lies within the WT distribution. If it is, then the same WT isolate may test resistant or susceptible on successive tests due to the inherent variability of testing.
2. Can an ECOFF be always discerned from the MIC distribution?
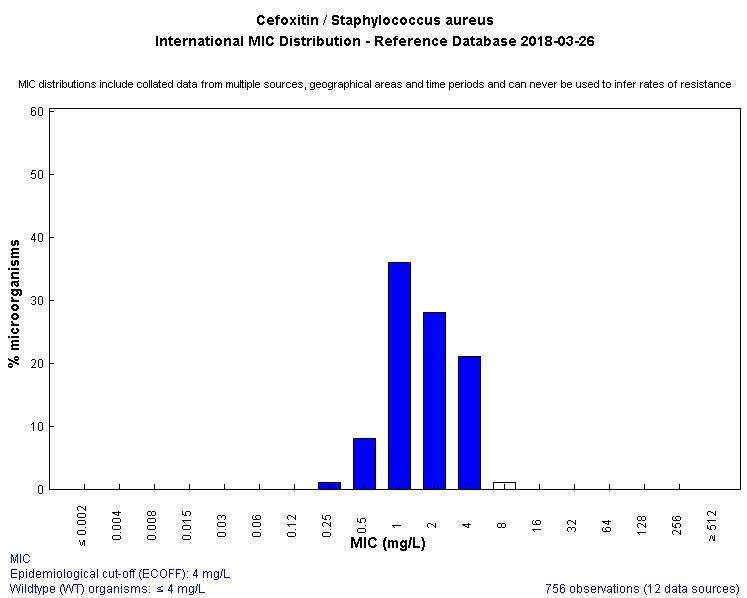
No- take a look at this distribution- the nonWT (red) isolates have a different MIC distribution but this overlaps the WT distribution. There is no MIC value that will separate the two populations. In this circumstance , provided the clinical breakpoint can be set above both distributions (i.e. achievable drug levels and PD parameters can be satisfied for isolates 2 or below) then there is no problem. Or perhaps a different antibiotic will allow the separation of WT and Non-WT – a good example is MRSA detection – the MIC distributions of MRSA and MSSA overlap when tested against oxacillin. When tested against cefoxitin, they dont overlap. See the following two graphics – WT is blue.


3. What quality control is necessary for AST? What are possible reasons for smaller or larger zones than expected when testing control organisms? How should one handle the control (ATCC) strains to ensure that they work properly?
Fiona’s presentations take you through what you need to know – please review them via here.
4. We discussed the three antimicrobial agents for this module – flucloxacillin, amoxycillin/clavulanate and cotrimoxazole (bactrim) which you need to systematically study. I asked whether Strep. pyogenes is ‘susceptible’ to cotrimoxazole (SXT)?
This recent paper provides one answer – S. pyogenes‘ in vitro susceptibility to SXT depends on the medium’s thymidine content and provided that is controlled, nearly all isolates are susceptible. There was a subsequent letter and reply which challenged the presumption that thymidine content in tissue may be sufficient to render SXT resistant in practice; however that is an issue that cannot be decided yet.
SXT remains useful for MSSA and MRSA treatment – the 2016 PMGH antibiogram showed 96% and 91% susceptibility for MSSA and MRSA respectively. Gram negative susceptibility unfortunately very low now.
This graphic about emergence of resistance in Staph. aureus is useful – Staph aureus resistance.
Please contact me with any other questions re this important topic. I will post a separate posting with questions on interpreting the cumulative antibiogram later this week. John
Module 1 2018 – additional short answer questions
- Contrast the terms phenotype versus genotype and give several examples related to antibiotic resistance in Staph. aureus and Coliforms.
- What does MLST stand for and how is it determined?
- What are disadvantages of using resistance genotype compared with a phenotype?
- Contrast the terms pharmacokinetics and pharmacodynamics when applied to antibiotics and their action against microorganisms.
- What does phylogeny mean?
References/reading
- New tree of life (Nature Microbiology 2012) – the phylogeny of life as shown by whole genome sequencing
- Microbiome review (BMJ 2017) – i will email you the pdf.
- WHO AMR Fact Sheet (Jan 2018)
Human Papilloma Virus key papers: testing strategy, impact of immunisation, women’s knowledge (PNG)
HPV and cervical cancer remain incredibly important topics for detailed study by all post graduates. Again, these papers are available as free text via the PUBMED links provided.
- Field Evaluation of Xpert HPV Point-of-Care Test for Detection of Human Papillomavirus Infection by Use of Self-Collected Vaginal and Clinician-Collected Cervical Specimens. J Clin Microbiol. 2016 Jul;54(7):1734-7. Toliman P et al.
An important paper to review: “Self-collected vaginal specimens had excellent agreement with clinician-collected cervical specimens for the detection of hrHPV infection using the Xpert HPV test. ”
[In other unpublished research from PNGIMR and Burnet Institute, abnormal acetic acid colposcopy-directed POC Xpert HPV testing was effective at enabling a same day cryotherapy approach to deal with HPV positive cervicopathology.
- Human papillomavirus vaccination: the population impact. Lee LY, Garland SM. F1000Res. 2017 Jun 12;6:866.An essential read – free full text and reasonably short. Provides an overview of all the HPV immunisation and its impact as a prophylactic measure, contrasting available data from around the world.
- Cervical Cancer Prevention Through HPV Vaccination in Low- and Middle-Income Countries in Asia Asian Pac J Cancer Prev. 2017 Sep 27;18(9):2339-2343.
“This mini-review focuses on the need for HPV vaccine implementation in Asia given the substantial disease burden and underuse of HPV vaccines in LMICs in this region. In addition, the progress towards HPV vaccine introduction, and barriers preventing further rollout of these essential, life-saving vaccines are also discussed in this article.”
- Ambiguous bodies, uncertain diseases: knowledge of cervical cancer in Papua New Guinea. Ethn Health. 2017 Feb 3:1-23. Kelly-Hanku A et al.
Very important qualitative research. “..found that knowledge and awareness about cervical cancer were poor … clear need to improve understanding of the female reproductive organs in order that people, women in particular, can be better informed about cervical cancer and ultimately better receptive to intervention strategies.”
The two yearly Pap test for women aged 18 to 69 will change to a five yearly human papillomavirus (HPV) test for women aged 25 to 74. Women will be due for the first Cervical Screening Test two years after their last Pap test. The changes include:
- women will be invited when they are due to participate via the National Cancer Screening Register
- the Pap smear will be replaced with the more accurate Cervical Screening Test
- the time between tests will change from two to five years
- the age at which screening starts will increase from 18 years to 25 years
- women aged 70 to 74 years will be invited to have an exit test.

STIs in the Pacific and elsewhere: some essential research papers to review
Most of these have free text available via the PUBMED link and come from projects lead by PNGIMR and the Kirby Institute. Remember as well to use the WHO STI Laboratory Manual as your microbiological study reference for these diseases and their diagnosis. If you have trouble getting the full papers, please contact me.
- A novel point-of-care testing strategy for sexually transmitted infections among pregnant women in high-burden settings: results of a feasibility study in Papua New Guinea. BMC Infect Dis. 2016 Jun 6;16:250. doi: 10.1186/s12879-016-1573-4.
The utility of the GenXpert platform for diagnosis of a range of STIs is apparent.
- Prevalence and risk factors of Chlamydia trachomatis, Neisseria gonorrhoeae, Trichomonas vaginalis and other sexually transmissible infections among women attending antenatal clinics in three provinces in Papua New Guinea: a cross-sectional survey . Sex Health. 2016 Oct;13(5):420-427. doi: 10.1071/SH15227.
- Prevalence and risk factors for Chlamydia trachomatis, Neisseria gonorrhoeae and Trichomonas vaginalis infection in pregnant women in Papua New Guinea. Sex Transm Infect. 2015 May;91(3):194-200. doi: 10.1136/sextrans-2014-051670. Epub 2014 Oct 13.
- Surveillance of antibiotic resistance in Neisseria gonorrhoeae in the WHO Western Pacific and South East Asian Regions, 2009. Commun Dis Intell Q Rep. 2011 Mar;35(1):2-7.
An important issue for laboratories in the Pacific – we need to ensure that culture methods are in place and that regular surveys of antimicrobial susceptibility take place- this enables appropriate guidelines to be put in place for drug supply and treatment.
-
High Proportion of Anorectal Chlamydia trachomatis and Neisseria gonorrhoeae After Routine Universal Urogenital and Anorectal Screening in Women Visiting the Sexually Transmitted Infection Clinic. van Liere GAFS, Dukers-Muijrers NHTM, Levels L, Hoebe CJPA. Clin Infect Dis. 2017 Jun 15;64(12):1705-1710.
The utility of routine testing of self-collected anorectal samples, even in clients who do not admit to anal intercourse.
- Dorsal longitudinal foreskin cut is associated with reduced risk of HIV, syphilis and genital herpes in men: a cross-sectional study in Papua New Guinea. J Int AIDS Soc. 2017 Apr 3;20(1):21358.
“In this large cross-sectional study, men with a dorsal longitudinal foreskin cut were significantly less likely to have HIV, HSV-2 and syphilis compared with uncut men, despite still having a complete (albeit morphologically altered) foreskin. …Exposure of the penile glans and inner foreskin appear to be key mechanisms by which male circumcision confers protection.”
Leishmaniasis case report and overview
- Case report, overview, diagnosis and treatment: Dr A Oon Leishmania July 2017
- Life cycle
- WHO Leishmaniasis site
From Stark et al, case report Medical Journal of Australia 2007 :
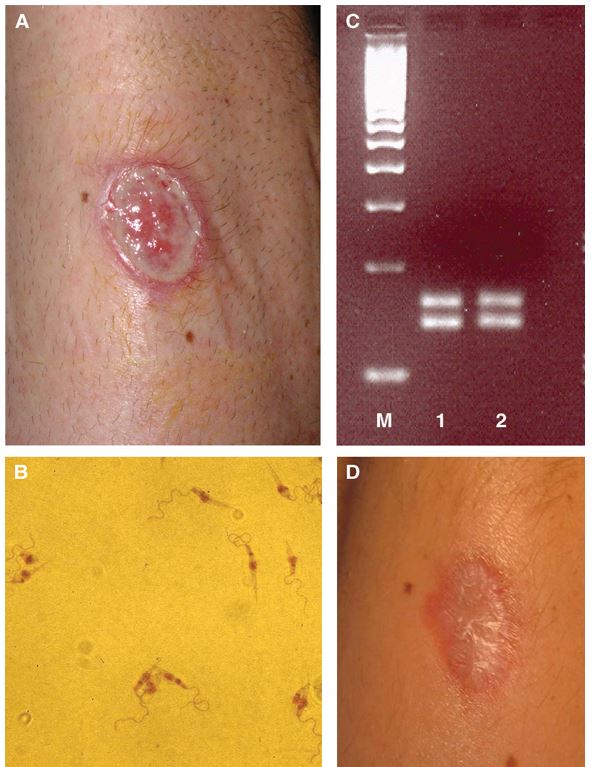
A: Non-healing New World cutaneous leishmaniasis ulcer on the left forearm.
B: Metacyclic Leishmania promastigotes in culture medium, Day 7.The parasites have a characteristic coiled, highly motile flagellum at the apical end of an elongated body (1020 mm in length) containing a round nucleus and rod-shaped kinetoplast.
C: Molecular banding pattern in agarose gel after PCR analysis. The banding pattern resulting from restriction fragment length polymorphism PCR analysis was consistent with Leishmania braziliensis DNA (M: a commercial 100-base-pair molecular marker [EZ Load 100 bp molecular ruler; Bio-Rad Laboratories, Hercules, Calif, USA]; 1: L. braziliensis control strain; 2: patient sample).
D: Healed ulcer, 4 weeks after treatment with amphotericin B.
Posted in Module - Parasitology, Nepal, Parasitology, Presentations
Tagged Leishmaniasis
Leave a comment
Toxoplasma, Amoebic meningoencephalitis & keratitis
Toxoplasmosis
- Overview- Toxoplasmosis
- Life cycle
Relevant manifestations to consider further:
- congenital – diagnosis – excellent recent guide
- reactivation in an immunocompromised (deficient cell-mediated immunity ) patient such as someone with advanced HIV – then cerebral abscess (may be multiple), retinitis or pneumonitis (similar picture to pneumocystis) occur – direct tissue demonstration of tachyzoites required generally (PCR also possible). Presumptive diagnosis usually made in HIV patient with cerebral abscess, usually after checking to confirm IgG seropositivity – therapeutic trial of antibiotic therapy then occurs – if no response then other differentials become more relevant – e.g. cerebral lymphoma.
Seroprevalence of anti-Toxoplasma gondii antibodies in HIV/AIDS patients and healthy blood donors at the Port Moresby General Hospital, Papua New Guinea.P N G Med J. 2012 Mar-Dec;55(1-4):88-93. 301 patients (181 HIV positive); overall antibody prevalence rate of 53% in the population and a significantly higher infection rate amongst HIV-positive patients.

Amoebic meningoencephalitis and keratitis
Primary amoebic meningoencephalitis in North Queensland: the paediatric experience. Med J Aust. 2016 Oct 3;205(7):325-8. Primary amoebic meningoencephalitis (PAM) is a fulminant, diffuse haemorrhagic meningoencephalitis caused by Naegleria fowleri, with an almost invariably fatal outcome. In Australia and the developed world, PAM remains a rare disease, although it is very likely that large numbers of cases go undetected in developing countries. N. fowleri is a thermophilic, free-living amoeba with a worldwide distribution. It is acquired when contaminated fresh water is flushed into the nose and penetrates the central nervous system via the cribriform plate. Clinical features are similar to those of bacterial meningitis, but it does not respond to standard therapy and rapid progression to death occurs in most cases. Some survivors have been reported; these patients received early treatment with amphotericin B in combination with a variety of other medications. Our review describes the local and worldwide experience of this disease and its clinical features, and discusses the associated diagnostic challenges. We hope that by detailing the local response to a recent case, and the outcomes of our public health campaign, we can improve the knowledge of this rare disease for doctors working in rural and remote Australia.
Primary amoebic meningoencephalitis in the Western Province. P N G Med J. 1991 Jun;34(2):87-9. Six cases of primary amoebic meningoencephalitis were diagnosed and treated at the Balimo Health Centre between December 1986 and September 1988. This disease has not previously been reported in Papua New Guinea although from information derived from other studies it should be occurring in the lowlands of Papua New Guinea from time to time. Although less than optimum treatment was given to the early cases the case fatality rate in the series was only 66%. This compares very favorably with a case fatality rate of nearly 100% from other studies. Early diagnosis and prompt treatment should help to reduce mortality.
Strategies for the prevention of contact lens-related Acanthamoeba keratitis. Ophthalmic Physiol Opt. 2016 Mar;36(2):77-92. Acanthamoeba keratitis is a severe, often sight threatening, corneal infection which in Western countries is predominantly seen in daily wear of contact lenses. This review aims to summarise the pathobiology and epidemiology of contact lens-related Acanthamoeba keratitis, and to present strategies for prevention, particularly with respect to modifiable risk factors in contact lens wear.
Posted in Module - Parasitology, Module-CNS infections, Parasitology
Tagged Amoebiasis, E. histolytica, Toxoplasmosis
Leave a comment
Coccidian enteric parasites- Cryptosporidium and Cyclospora
FERGUSON 2011 Coccidian enteric parasites (includes references relevant to Nepal)
- Rapid diagnostic tests for Cryptosporidium are effective- often combined with a giardia test. However as the illness is self-limited in the immunocompetent, testing probably not relevant. Highly relevant for immunocompromised patients where treatment is required.
- Life cycle of Cryptosporidium.
- Two PNG- associated references:
Seroepidemiology of cryptosporidiosis in children in Papua New Guinea and Australia.Groves VJ1, Lehmann D, Gilbert GL. Epidemiol Infect. 1994 Dec;113(3):491-9.
Enzyme immunoassays (EIA) were used to measure serum antibodies to Cryptosporidium in four immunocompetent adults with recent proven cryptosporidial infection, 379 healthy children and 73 adult volunteers in Melbourne, Australia, and 205 children in Papua New Guinea (PNG) (47 healthy children; 158 with pneumonia). Antibodies peaked 3-6 weeks after infection and fell to baseline within a few months. A high level (5000 EIA units/ml) or a significant change between paired sera, of IgG or IgM, were taken as evidence of recent infection and found in 24% of PNG children and in 8% of children and 5% of adults in Melbourne. Among PNG children with pneumonia who had high cryptosporidial antibody levels, those with measles (6/8) were significantly more likely (P = 0.002) to have diarrhoea than the remainder (4/28). Symptomatic cryptosporidiosis may be associated with transient immune suppression due to viral infection. This study indicates that serological surveys can contribute to an understanding of the epidemiology of cryptosporidosis.
Cryptosporidium species in sheep and goats from Papua New Guinea. Exp Parasitol. 2014 Jun;141:134-7.
Species of Cryptosporidium are extensively recognised as pathogens of domesticated livestock and poultry, companion animals, wildlife, and are a threat to public health. Little is known of the prevalence of Cryptosporidium spp. in humans, domesticated animals or wildlife in Papua New Guinea (PNG). The aim of the present study was to screen sheep and goats for Cryptosporidium using molecular tools. A total of 504 faecal samples were collected from sheep (n=276) and goats (n=228) in village, government and institutional farms in PNG. Samples were screened by nested PCR and genotyped at the 18S rRNA and at the 60kDa glycoprotein (gp60) loci. The overall prevalences were 2.2% for sheep (6/278) and 4.4% (10/228) for goats. The species/genotypes identified were Cryptosporidium hominis (subtype IdA15G1) in goats (n=6), Cryptosporidium parvum (subtypes IIaA15G2R1and IIaA19G4R1) in sheep (n=4) and in goats (n=2), Cryptosporidium andersoni (n=1) and Cryptosporidium scrofarum (n=1) in sheep, Cryptosporidium xiao (n=1) and Cryptosporidium rat genotype II (n=1) in goats. This is the first report of Cryptosporidium spp. identified in sheep and goats in PNG. Identification of Cryptosporidium in livestock warrants better care of farm animals to avoid contamination and illness in vulnerable population. The detection of zoonotic Cryptosporidium in livestock suggests these animals may serve as reservoirs for human infection.

{kind=link}
{kind=link}
{kind=link}